
OnSTAFF 2000
Charges /Encounter/Add.
General Information Regarding Encounter Screens
There are three types of encounter screens: Encounter, Worker’s Comp Encounter and UB Encounter. These screens serve several purposes. They allow entry of additional claim information such as authorization numbers, information for attorney, lien or worker's comp cases, hospital admission and discharge dates and more. This information is stored for later retrieval.
Encounters:
When the patient has an insurance category type, an encounter may be added, modified or viewed through Main Menu/New Patient/Add, Modify or View.
NOTE: Main Menu/New Patient/Add allows adding encounter information upon registering a new patient. After exiting the Add New Patient mode, encounters may only be added through Main Menu/Charges /Encounter/Add.
Independent of the patient’s category type, an encounter may be added, modified, viewed or deleted through Main Menu/Charges/Encounter/Add, Modify, View or Delete.
Worker’s Comp Encounters:
When the patient has a worker’s comp category type, a worker’s comp encounter may be accessed only through Main Menu/New Patient/Add, Modify or View.
UB Encounters:
Independent of the patient’s category type, UB encounters may only be added, modified, viewed or deleted through Main Menu/Charges/UB Encounter/Add/Modify/View or Delete.
See NOTE regarding category types.
Encounter Information
When the Encounter option is selected from the Charge Menu, On-Staff will display the following:
ENCOUNTER/CLAIM INFORMATION
Add Modify View Delete Exit
When selecting the Add option, On-Staff will display the following encounter screen:
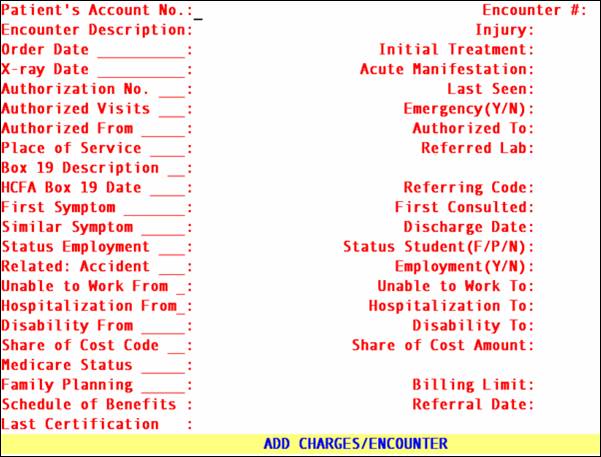
Patient's
Account No.: When not already displayed, enter the patient’s account number. If the account number is unknown, you may search by entering all or part of the name (last name, first name) and/or incorporating the Wild Card (*) and press the [F2] search key.
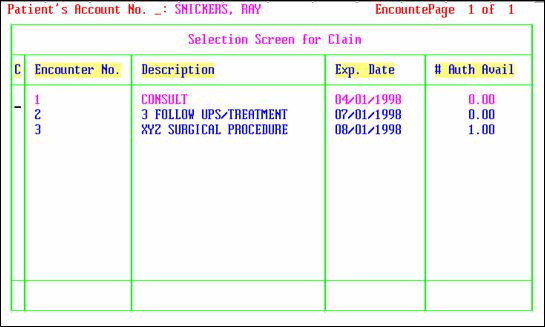
Encounter #: This number is assigned automatically when adding a new record. When this information is modified later, the number of each encounter may be retrieved individually. When the encounter number is unknown, clear the field by pressing the [Spacebar] then press the [F2] search key to display the Selection Screen for Claim. When [F2] is pressed again, ALL encounters entered for that patient will be displayed (see following example). To select an encounter, move the cursor to highlight the desired one and press [Enter]. To exit this screen without making a selection, from the C (command) column press Q or [End].
Encounter
Description: Enter the description of this encounter for later reference. Enter as much information as to be helpful in selecting the correct encounter to attach to a charge.
Injury Date For Workers Comp patients will print in Box 14 of the HCFA 1500 claim form only when the patient’s category type is worker’s comp (/Utility/Category <Type (C/P/W/O/F/G)> W or F).

For electronic claims submission Loop 2300 DTP 439.
Order Date: Type the date for claims that include an order (order for service or supplies to
be billed and/or reported).For electronic claims submission Loop 2300 DTP*180.
Initial Treatment: Type the date of initial treatment for claims involving spinal manipulation. Required for spinal manipulations. When submitting this information electronically, this date is required at the 2300-DTP 454 segment.
X-Ray Date: Type the date of "Last X-ray" for spinal manipulation. Date will be found in Loop 2400 DTP*455.
Manifestation: Used for Electronic submission of claims involving spinal manipulation with Medicare coverage. Required for electronic claim submission when Loop 2300 CR208 = “A” or “M,” the claim involves spinal manipulation, and the payer is Medicare. Date will be found in Loop 2300 DTP*453*.
No.: Enter the authorization number issued by private insurance companies (i.e., an HMO tar number) for the treatment given under this encounter. This information will print in Box 23 of the HCFA 1500 claim form and will be transmitted electronically for all insurance types other than Medi-Cal (/Utility/Insurance <Insurance Type> does not equal D).
Last Seen: Type the date the patient was last seen by the attending physician for the qualifying condition related to the services performed. This is a required field when services involve an independent PT, an occupational therapist or physician involving routine foot care. Intellect will complete box 14 HCFA (CMS 1500). Or used for electronic claim submission Loop 2300 DTP*304*D8*.
Authorized
Visits: Enter the number of visits the insurance company authorized for the treatment given under this encounter. This field will decrement the number for each unique service date as charges are posted to this encounter. When the encounter number is entered on the Charge Screen and [Enter] has been pressed, the number of remaining authorized visits will be displayed. Only whole numbers should be used (i.e., 1, 2, 10). This field will accept numbers such as 10.30 but the .30 will not be recognized.
Emergency (Y/N) Enter “Y” or “N” yes or no for emergency. System places a “Y” only in box 24 C. HCFA (CMS 1500)

Or used for electronic claim submission Loop 2400 SV109.
Authorized
From: / To: Enter the beginning and ending effective dates the insurance company authorized for the treatment given under this encounter. When posting charges with this encounter and the date of service is not within this range, On-Staff will allow the user to continue posting but will display the following warning:
WARNING
Date Of Service Is Not Within The
Authorized Dates Set In Encounter Screen.
Press Any Key To Continue.
Service: This is an informational field only and does not print anywhere. For reference, enter the /Utility/Facility <Facility Code> that designates the place of service where the service has been authorized to be rendered (when this is other than the office). When the code is unknown, the [F2] search key may be used.
.
Lab: Used only for lab work done outside the office which your office will be billing the patient’s insurance for and the lab will be billing you. Enter the /Utility/Referring <Referring Code> that designates the appropriate outside lab. When the code is unknown, the [F2] search key may be used. When software requirements are met, the lab name and address will print in Box 32 of the HCFA 1500 claim form.
![]()
D Description: This is a thirty character, free form comment field that will print in Box 19 of the HCFA 1500 claim form.
![]()
H HCFA Box 19
D Date: This is a date field which will print in Box 19 of the HCFA 1500 claim form.
R Referring Code:
First Symptom: Enter the date of the first symptom. This date will print in Box 14 of the HCFA 1500 claim form only when the patient’s category type is other than worker’s comp (/Utility/Category <Type (C/P/W/O/F/G)> does not equal W or F).
![]()
Or used for electronic claims submission Loop 2400 DTP*431*D8*.
Consulted: Enter the date of the first consultation. This date will print in Box 15 of the HCFA 1500 claim form only when the patient’s insurance type is other than Medicare, Medi-Medi or Medi-Cal (Medi-Caid) (/Utility/Insurance <Insurance Type> does not equal C, 1, or D).
![]()
Similar Symptom If the patient has had similar symptoms in the past, enter Y in this field. This is an informational field only and does not print anywhere.
Discharge Date: Enter the date the patient was released from the doctor’s care for the above injury or accident. This date will print on attorney statements printed through /Billing/Worker/Attorney when the patient’s category type is worker’s comp (/Utility/Category <Type (C/P/W/O/F/G)> W or F).
Employment: Enter the employment status of the patient. Indicating full or part time employment will print an x in the Employed Box of 8 on the HCFA 1500 claim form. Pressing the [F2] search key will display the following valid choices:
F Full Time
P Part Time
N Unemployed

(F/P/N): Enter the student status of the patient. This field’s entry will print an x either in the Full-Time or Part-Time Student in Box 8 of the HCFA 1500 claim form. Pressing the [F2] search key will display the following valid choices:
F Full Time
P Part Time
N Not Enrolled

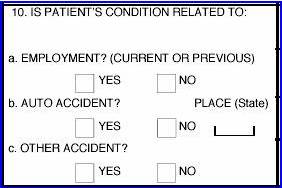
(A/O/N): Indicate the origin of the above injury or accident. This field’s entry will print an x in the YES or NO Box of 10b or c on the HCFA 1500 claim form. Pressing the [F2] search key will display the following valid choices:
A Related to automobile accident
O Related to other type of accident
N Not related to an accident (default value)

Or Electronic claims submission Loop 2300 CLM11 - 1 through CLM11 - 3:
AA Auto Accident
AB Abuse
AP Another Party Responsible
EM Employment
OA Other Accident
(Y/N): Indicate “Y” or “N” Whether condition is related to employment. Will place an “X” in box 10a HCFA (CMS 1500).
Or electronic claims submission Loop 2300 CLM11 - 1 through CLM11 - 3:
AA Auto Accident
AB Abuse
AP Another Party Responsible
EM Employment
OA Other Accident
Work From: Enter the beginning date this patient was unable to work. This will print in Box 16 of the HCFA 1500 claim form.

Unable To
Work To: Enter the ending date this patient was unable to work. This will print in Box 16 of the HCFA 1500 claim form.
From: Enter the admit date regarding hospitalization of the patient. This information will print in Box 18 of the HCFA 1500 claim form.
Or used for electronic claims submission Loop 2400 DTP*435*D8*.
Hospitalization
To: Enter the discharge date regarding hospitalization of the patient. This information will print in Box 18 of the HCFA 1500 claim
![]()
Or used for electronic claims submission Loop 2400 DTP*096*D8*.
From Type date disability began. Replaces <Unable To Work From> on the CMS 1500 (HCFA) for students, unemployed, or persons unable to do their current job. Used in electronic claims processing Loop 2300 DTP*360*D8.
Disability
To Type date able to return full work if applicable. Replaces <Unable To Work From> on the CMS 1500 (HCFA) for students, unemployed, or persons unable to do their current job. Used in electronic claims processing Loop 2300 DTP*361*D8
The following Share of Cost Code and Share of Cost Amount fields are for Medi-Cal (Medi-Caid) patient’s only (/Utility/Insurance <Type> = D).
Code: This is an informational field only and does not print anywhere. Enter the Medi-Cal share of cost code for this patient.
Share of Cost
Amount: If Medi-Cal is primary (Utility/ Insurance <Insurance Type> =D), Intellect will complete box 10 d HCFA CMS 1500 with this amount.
![]()
Status: Used only with Medi-Cal patient’s who fall into the category of Alien Residents of Medicare Eligibility Age but do not have Medicare coverage. Consult your Medi-Cal billing manual for further instructions. This field’s entry will print in Box 22 of the HCFA 1500 claim form only when the patient’s insurance type is Medi-Cal (Medi-Caid) or Medi-Medi (/Utility/Insurance <Type> = D or 1).

Family Planning For MCAL patients enter the appropriate code. Will complete box 24H HCFA (CMS 1500).
![]()
Billing Limit Enter the appropriate Delay Reason Code.
Schedule of Benefits Used with GTE Electronic Billing. Enter the code given by the insurance company at the time of verifying eligibility (when applicable). This may be used as an informational field by your practice. This field does not print anywhere.
Referral Date
Last Certification If therapy involved, type the date the therapist was last certified. Used in electronic billing
After the last field has been entered, the cursor will return to the Encounter Description field allowing the user to review the accuracy of the entered data. When satisfied, to exit this process press [“] or [End].